 Illinois is considering HB 218, a measure that would decriminalize marijuana. While this may be a laudable goal, HB 218 achieves its objective by throwing victims of stoned driving under the bus. Illinois currently is blessed with one of the strongest DUI-D laws in the nation, based on a defensible zero tolerance policy. HB 218 would remove THC’s zero tolerance policy and replace it with a per se standard of 15 ng/ml in blood for marijuana’s impairing delta-9-tetrahydrocannabinol (THC). No, that’s not a typo. If passed into law, this would be the highest THC per se standard in the nation.
Illinois is considering HB 218, a measure that would decriminalize marijuana. While this may be a laudable goal, HB 218 achieves its objective by throwing victims of stoned driving under the bus. Illinois currently is blessed with one of the strongest DUI-D laws in the nation, based on a defensible zero tolerance policy. HB 218 would remove THC’s zero tolerance policy and replace it with a per se standard of 15 ng/ml in blood for marijuana’s impairing delta-9-tetrahydrocannabinol (THC). No, that’s not a typo. If passed into law, this would be the highest THC per se standard in the nation.
The bill drafter’s rationale for the nation’s highest THC per se limit is:
- If we’re going to decriminalize marijuana, we cannot have a zero tolerance policy for driving under the influence of marijuana.
- A 15 ng/ml THC per se standard will protect public safety. A 15 ng/ml in blood standard for marijuana’s impairing delta-9-tetrahydrocannabinol (THC) is supported by scientific research.
- Drivers under the influence of marijuana who test below 15 ng/ml THC in blood can still be prosecuted for DUI-D under Illinois’ impairment statute.
Not one of the above claims is true.
Point No. 1: Decriminalization and Zero Tolerance Are Compatible
Arizona, Georgia, Utah, Iowa, Rhode Island, North Carolina, South Dakota, Delaware. Pennsylvania, Indiana, Wisconsin and Michigan have zero tolerance for many substances, including THC. Many of these states permit the use of marijuana for medicinal purposes, making it legal in those states.
A zero tolerance policy does not criminalize the mere presence of illegal drugs in a driver. The driver must first be apprehended for probable cause of driving under the influence of drugs. Statutes can make this crystal clear, as has been done in New Zealand’s national laws.
If a state chooses to use a per se THC standard, rather than a zero tolerance policy to ensure the public is protected from DUI-D drivers, it can do so with a THC level that actually protects the public, as is done in Nevada and Ohio, both of which have THC per se limits of 2 ng/ml THC in whole blood. England and Wales did the same last year.
The reason zero tolerance policies are preferred over per se limits to deal with THC-impaired driving is that there is no level of THC above which, everyone is impaired, and below which, no one is impaired. This is not because we need more studies; it’s the nature of human biology. THC is unlike alcohol chemically, biologically and metabolically, so it should come as no surprise that successful strategies to deal with drunk driving won’t work as successfully with THC-impaired driving.
Point No. 2: A 15 ng THC standard will harm public safety, and is not scientifically based
No one in the world has used a THC per se standard as high as 15 ng/ml in blood. The highest standard used is in Colorado, Washington and Montana, all of which adopted 5 ng/ml THC in whole blood, against the advice of toxicologists who cautioned that such a number was far too high.
NMS Labs, a nationally recognized forensic toxicology laboratory recently published laboratory test data on 10,144 Marijuana DUID/DRE cases that tested positive for cannabinoids, either THC, its inactive metabolite, or both. In each case, DREs believed the evidence at the scene was sufficient to justify the expense of a laboratory test to confirm the presence of THC. 70.4% of those cases tested below 5 ng/ml THC in blood.
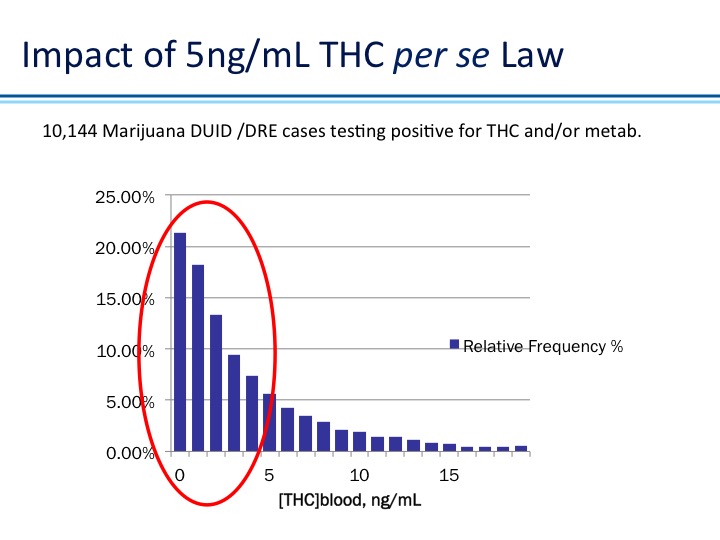
An extremely small percentage, under 3%, tested above 15 ng/ml.
European experiments have confirmed that THC impairment begins at 1-2 ng/ml THC in whole blood, but not for everyone. It’s the latter caution “but not for everyone” that leads the marijuana lobby to demand a THC standard well above the 5 ng/ml standard that is proving ineffective in other states. They prefer a 15-25 ng/ml THC in whole blood level because even the most extreme marijuana addict is believed to be impaired at those levels. The problem, of course, is that 97% or higher of everyone else is impaired at levels well under those extreme per se levels.
THC and alcohol do not impair either blood or oral fluid. They only impair the brain. We can only test drugs in the brain by means of an autopsy, something most drivers would find objectionable. Blood is tested as a surrogate to estimate what is in the brain. For alcohol, blood is an excellent surrogate. Alcohol is a small, water soluble molecule that rapidly equilibrates between the blood and the brain by easily crossing the blood:brain barrier. Therefore, what’s in the blood is in the brain, and vice-versa. For THC, blood is a terrible surrogate since THC is a very much larger, fat-soluble molecule. There is very little correlation between THC blood concentration and THC brain concentration. After smoking a joint, THC concentration in the brain rises at the same time as its concentration in the blood is falling. So it should come as no surprise that there is little correlation between THC blood concentration and driving impairment.
Much less is known about correlation of THC in oral fluid with either THC in the brain or with driving impairment. We do know that the correlation between THC oral fluid concentration and THC blood concentration is irregular, and that THC levels in oral fluid are generally very much higher than THC levels in the blood, by a factor of 10, 20 30 or more depending upon many variables. A level of 25 ng/ml THC in oral fluid can be the equivalent of less than 1 ng/ml THC in blood (J.G. Ramaekers et al., Drug and Alcohol Dependence 85 (2006) 114–122).
European experiments simultaneously measured impairment and blood concentration, something that cannot be done in real-world traffic safety management situations. In Colorado we find that the normal time between a proactive stop and taking of a blood sample for testing is just over 1 hour. It’s over 2 hours if it’s a reactive arrest for a crash, and 3 1/2 hours if a warrant is required. These times are material, since 90% of marijuana’s THC is cleared from the blood within the first hour after smoking. This is one reason why the NMS labs data shows what it does.
Point No. 3 Stoned Drivers below 15 ng will not be prosecuted for DUI-D
A per se standard would preclude successful prosecution under an impairment standard. Illinois is one of 12 states that statutorily define DUI as “incapable of driving safely,” contrasted with Washington, for example, where the statute says DUI means “affected by, exhibited effects of consumption.” The reason alcohol per se laws were put in place was because of the profound difficulty of proving someone was incapable of driving safely. Some people can drive safely with a BAC above the .08 standard, but many are impaired at a BAC below .08, which is why the alcohol per se standard is set at .05 BAC in many other countries. So ask yourself, ”How many Illinois DUI alcohol defendants are convicted of DUI when they have a BAC below .08?” It almost never happens. So why would we expect stoned drivers testing below 15 ng/ml THC to be successfully prosecuted for DUI-D?